There is no single test that can either establish or exclude ARVC/D. The criteria that are used to determine ARVC/D include a physical examination, family history of the disease, various cardiac tests, and genetic information.
Diagnosing ARVC/D
In 1994, an International Task Force proposed criteria for the clinical diagnosis of ARVC/D, based on structural, electrocardiographic, arrhythmic, histological and familial characteristics of ARVC/D. These diagnostic criteria were revised in 2010 and now incorporate advances in both technology and genetics.
The diagnosis of ARVC/D consists of a combination of the Task Force Criteria from different categories that are classified as a major or minor.
Evaluating patients
Patients evaluated using the criteria above may be classified as “definite,” “probable,” or “possible” sufferers of ARVC/D. Patients may also not have sufficient criteria to establish a definite diagnosis, in which case they may be classified as “borderline” for being affected or “possible” for having the disease.
Evaluating family members
To evaluate family members of individuals known to have ARVC/D, use the Hamid assessment criteria in this study [PDF] (J Am Coll Cardiol. 2002; 40: 1445–1450).
Symptoms
- Arrhythmias:
- PVCs
- Nonsustained VT
- Sustained VT of left bundle morphology
- Syncope
- Heart failure
- Sudden cardiac arrest
Differential diagnosis
The major condition which needs to be differentiated from ARVC/D is idiopathic ventricular tachycardia arising from the outflow tract. The ECG appearance of the ventricular tachycardia can be similar, but there is no structural abnormality of the heart; this is unlike the situation in ARVC/D where commonly there is dilatation, abnormal contraction, or reduced function of the right ventricle.
Right ventricular outflow tract tachycardia (RVOT) is more common than ARVC/D and occurs in young, otherwise healthy people. The treatment is either with medications or with catheter ablation.
Tests
Tests may include the following:
- Electrocardiogram
- Signal Averaged Electrocardiogram
- 24-hour Holter Monitor
- Exercise Stress Test
- Electrophysiology Study
- Genetic Testing
- Echocardiogram (Imaging)
- Cardiac Magnetic Resonance (MRI) (Imaging)
- Cardiac Computed Tomography (CT) (Imaging)
- Right Ventriculogram (RV angiogram) (Imaging)
- Cardiac Biopsy
Electrocardiography
A standard 12-lead electrocardiogram (ECG) is a useful diagnostic tool to evaluate a patient for ARVC/D. There are 4 main diagnostic ECG characteristics one should assess:
- T-wave inversions in the precordial leads
- Epsilon waves
- Terminal activation delay (TAD)
- T-wave changes in right bundle branch block (RBBB)
We suggest obtaining a 12-lead ECG using standard recording techniques (paper speed: 25 mm/s; 1 mm amplitude = 1 mV; 150 Hz filter).
Repolarization Abnormalities
The presence of T-wave inversions in leads V1-V3 or beyond in the absence of a complete right bundle branch block (QRS≥120 ms) represents a major criterion according to the 2010 Diagnostic Task Force Criteria. T-wave inversions in leads V1 and V2 in the absence of a complete right bundle branch block or in leads V1-V4 in the presence of a complete right bundle branch block represent a minor criterion.
We find that T-wave inversions are an important parameter as they are easy to recognize and require no special measurement.
Depolarization Abnormalities
A more difficult ECG characteristic to identify is the epsilon wave which represents a major criterion. The epsilon wave is defined as “waves of small amplitude that occupies the ST segment in the right precordial leads and is distinct from the QRS complex.” Epsilon waves are seen more frequently in patients with severe disease where the diagnosis is rarely uncertain.
Terminal Activation Delay (TAD) is defined as “the duration of the terminal part of the QRS complex from the nadir of the S wave to the end of all depolarization in V1 –V3. A TAD of ≥55ms in the absence of a complete right bundle branch block constitutes a minor criterion.” Although this is a valuable addition to the diagnostic criteria, the error with which precise time measurements are made on ECG tracings results in the criterion being less reproducible and more difficult to apply.
A Signal Averaged Electrocardiogram (SAECG) is another diagnostic tool used to assess depolarization abnormalities in ARVC/D when the QRS duration is ≤110ms on a standard ECG. Late potentials observed in one or more parameters (filtered QRS, LAS duration or RMS voltage of terminal 40ms) represent a minor criterion. We recommend averaging 350 beats at a filter setting of 40-250 Hz with a noise level < 0.3uV. It is preferable to obtain two separate SAECGS in order to be certain of the results.
If a patient has a complete RBBB pattern, none of the SAECG parameters listed above can be used to make the diagnosis of ARVC/D. Patients with ARVC/D and RBBB may have extensive T-wave inversions across the precordium extending beyond V3 and an R’/S ratio < 1 in lead V1.
Only one of these criteria including that for RBBB, epsilon wave, TAD or SAECG can be applied toward the diagnostic criteria.
Arrhythmias
Arrhythmias in patients with ARVC/D may be observed on a 12-lead ECG, exercise stress test, Holter or event monitor. A 24-hour Holter can document the frequency and types of arrhythmias, even in asymptomatic patients.
Diagnostic arrhythmia criteria for probands can be met by the presence of >500 ventricular extrasystoles within a 24-hour time period (minor criteria). It is important to assess the morphology of VT, as this can determine if the VT is a major or minor criterion. VT of a left bundle superior axis (nonsustained or sustained) with a negative or indeterminate QRS in II, III, and a VF and positive in AVL is considered a major criteria. Nonsustained or sustained VT of left bundle inferior axis, or sustained VT of unknown axis is a minor criterion.
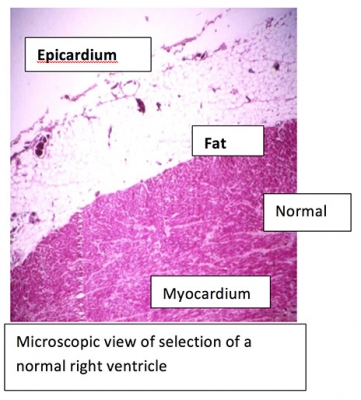
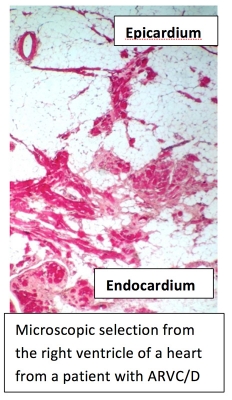
Imaging
The right ventricle is of primary interest when assessing for ARVC/D. The right ventricular structure and function can be observed by echocardiogram, MRI, CT scan and/or angiogram. The presence of abnormal contraction of the right ventricle (akinesis/dyskinesia/or aneurysm) on Echo or MRI is not sufficient by itself to meet the diagnostic criteria for ARVC/D. Other measurements that quantitate RV enlargement also need to be met. Specific protocols have been developed to focus attention on imaging the right ventricle.